The History of Brachioplasty (Arm Lift) Surgery
Brachioplasty has evolved over nearly a century. Early descriptions in the 1930s focused on removing excess tissue of the upper arm. Over time, surgeons explored new incision patterns, improved understanding of the superficial fascial system, and integrated suction‑assisted lipectomy to address excess fat. The goal across eras has been consistent: to manage excess skin and fatty tissue of the upper arm in a way that balances function, safety, and scar placement. Techniques continue to be refined as evidence and technology advance.
Important: Surgery has risks and outcomes vary. Decisions should be based on a consultation with a suitably qualified specialist surgeon (FRACS) who can assess individual goals, medical history, and suitability for surgery.

Timeline of Key Publications and Technique Descriptions
(Numbers in brackets refer to the reference list below.)
- 1930 – Thorek: Early description of upper‑arm reduction in women with excess tissue. (24, 30, 32)
- 1943 – Posse: Elliptical incision approach. (24, 27, 30)
- 1954 – Correa‑Iturraspè & Fernandez: First aesthetic arm lift (brachioplasty) description. (9, 24, 30)
- 1973 – Lewis: Z‑plasty carried into the axilla to address scar line irregularity. (24, 30)
- 1975 – Pitanguy: S‑shaped incision variant. (24, 25, 30)
- 1975 – Arpad & Fischer: Introduction of modern suction‑assisted lipectomy (liposuction) techniques. (5, 13, 30)
- 1977 – Pitanguy: “Bat‑wing torsoplasty” extending into the axilla for redundant skin. (24, 26, 30)
- 1977 – Franco & Rebello: L‑shaped incision. (14, 30)
- 1979 – Guerrero‑Santos: Lenticular excision. (17, 30)
- 1979 – Juri: Quadrangular flap with T‑closure. (19, 30)
- 1980 – Regnault: Fishtail‑variant incision. (29, 30)
- 1982 – Borges: W‑plasty incision. (6, 30)
- 1983 – Regnault: Axilloplasty concepts for excess axillary skin. (28, 30)
- 1985 – Avelar: Addition of liposuction to body‑contouring procedures reported. (30)
- 1989 – Goddio: Deepithelialisation and repositioning of the posterior arm flap to create a bicipital groove. (16, 30)
- 1995 – Lockwood: Superficial fascial system (SFS) suspension. (22, 30)
- 1996 – Marques: Excision addressing brachium, axilla and elbow in one procedure. (23, 30)
- 1997 – Gilliland & Lyos: CAST liposuction as an alternative in selected patients. (15, 30)
- 2000 – de Souza Pinto: S‑shaped moulds to guide symmetric excision. (10, 30)
- 2001 – Richards: Minimal‑incision brachioplasty (axillary‑based scar) for carefully selected cases. (30)
- 2004 – Strauch: Sinusoidal posterior‑arm incision with axillary Z‑plasty. (30, 31)
- 2006 – Chandawarkar: Fish‑incision variant. (8, 30)
- 2006 – Aly: Double‑ellipse incision; and Aly T‑brachioplasty. (3, 4, 30)
- 2006 – Hurwitz: Inverted L‑shaped incision. (18, 30)
- 2007 – Hoyos & Millard: VASER liposuction (ultrasound‑assisted) described. (2)
- 2013 – Aboul Wafa: Medial S‑shaped incision to reduce contracture. (1, 30)
- 2013 – Bracaglia: “Kris‑knife” incision variant. (7, 30)
- 2014 – Knotts: Avulsion brachioplasty with liposuction within the planned ellipse. (20, 30)
- 2014 – Fantozzi: BTV (balanced triple‑vector) approach with dual‑opposing flaps. (11, 30)
- 2014 – Kornstein: Fascial support using silk‑derived scaffold (SERI) adjunct. (21, 30)
- 2015 – Ferraro: Modified fish‑tail incision to address axillary contour. (12, 30)
Early Concepts (1930–1954)
- 1930: Thorek described aesthetic surgery of the arms in women with excess tissue. (24, 30, 32)
- 1943: Posse reported elliptical excisions in obese patients. (24, 27, 30)
- 1954: Correa‑Iturraspè and Fernandez provided the first aesthetic description of brachioplasty. (9)
Expanding Incision Designs (1973–1980)
Through the 1970s and into 1980, surgeons explored Z‑plasty, S‑shaped, L‑shaped, lenticular and T‑closure patterns to relocate tension lines and manage axillary redundancy. (14, 17, 19, 24, 25, 29, 30)
Liposuction Enters the Field (mid‑1970s onward)
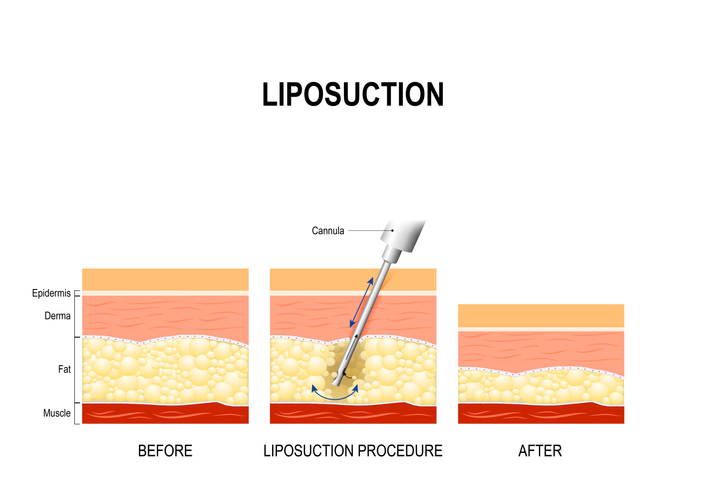
Modern suction‑assisted lipectomy (liposuction) emerged in the mid‑1970s and was progressively combined with body‑contouring procedures. (5, 13, 30) Integration with brachioplasty accelerated in the 1980s and 1990s as techniques and safety protocols matured. (30)
Refinements of the 1980s–1990s
- Incision strategy and axillary management: Regnault (fishtail; axilloplasty) and Borges (W‑plasty) contributed patterns still referenced today. (6, 28–30)
- Contour‑support concepts: Goddio described deepithelialisation/repositioning of the posterior flap to define the bicipital groove. (16, 30)
- SFS suspension: Lockwood’s work on suspending the superficial fascial system sought consistent contour and scar behaviour. (22, 30)
- Alternatives in selected cases: CAST liposuction (Gilliland & Lyos) described circumferential para‑axillary superficial tumescent liposuction, with mixed outcomes and complications including seroma in a subset. (15, 30)
2000s: Symmetry, Scar Placement and Axillary Contour
- Templates and planning: de Souza Pinto et al. used S‑shaped moulds to assist scar symmetry. (10, 30)
- Minimal‑incision options: Richards described axillary‑based minimal‑incision approaches for mild laxity; patient selection is critical. (30)
- Posterior‑arm sinusoidal incision: Strauch et al. proposed a curved line with axillary Z‑plasty to help camouflage the scar and reduce contracture risk. (30, 31)
- Pattern exploration: Fish‑incision (Chandawarkar), double‑ellipse and T‑brachioplasty (Aly), and inverted‑L (Hurwitz) broadened the toolkit. (3, 4, 8, 18, 30)
2007 onwards: Ultrasound‑Assisted Liposuction and Contemporary Variations
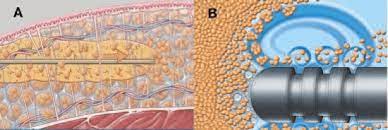
- VASER liposuction (ultrasound‑assisted): Described by Hoyos and Millard; some surgeons use this technology when combining liposuction with brachioplasty. (2)
- 2013–2015 technique reports: Medial S‑incisions (Aboul Wafa), kris‑knife (Bracaglia), avulsion brachioplasty with integrated liposuction (Knotts), BTV dual‑flap strategy (Fantozzi), fascial support with SERI (Kornstein), and modified fish‑tail to address axillary contour (Ferraro). (1, 7, 11, 12, 20, 21, 30)
What This Means for Patients Today
Face blurred for privacy
Disclaimer: Operation performed by Dr Bernard Beldholm. Adult content, surgery has risks; individual results vary, seek 2nd opinion. Please see the full disclaimer.
- Personalised planning: Technique selection depends on skin quality, distribution of excess tissue, presence of axillary redundancy, and patient priorities regarding scar placement and recovery.
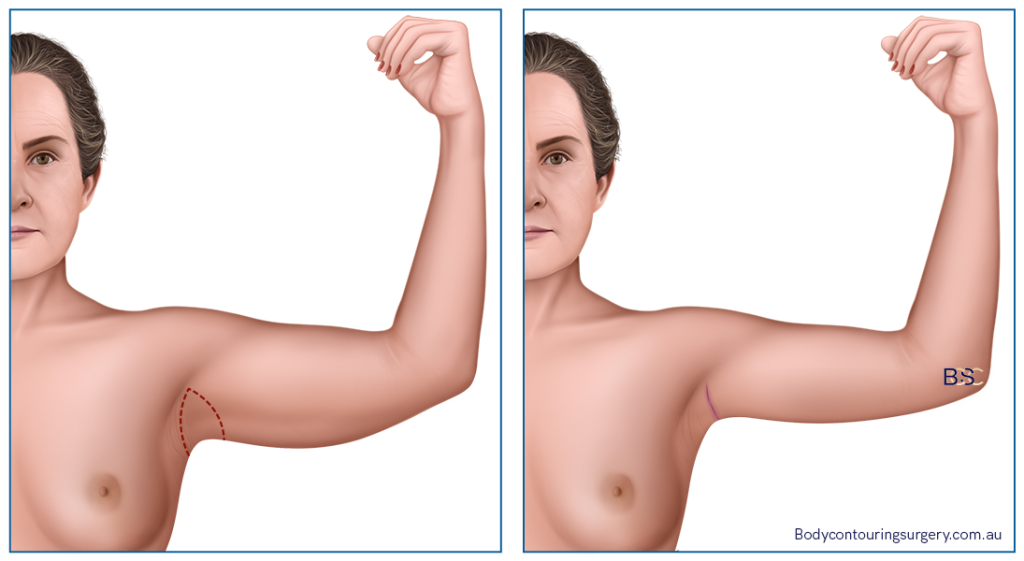
- Scars are inherent: All brachioplasty methods involve scars. Incision design aims to place scars as discreetly as anatomy allows, but visibility varies between individuals.
- Combination with liposuction: In suitable patients, adding liposuction (suction‑assisted lipectomy) can address localised fat. Whether to use standard or ultrasound‑assisted methods (e.g., VASER) is a clinical decision made with the treating surgeon.
- Safety: Reported complications include issues such as seroma, wound problems, altered sensation (e.g., medial brachial cutaneous nerve injury), and general surgical/anaesthetic risks. Published rates vary by technique and patient factors. (15, 21, 30)
Reminder: This page is general information and not a substitute for individual medical advice. Outcomes and recovery differ between people.
References
- Aboul Wafa AM. S‑shaped brachioplasty… Plast Reconstr Surg. 2013;131:661e–3e.
- Hoyos AE, Millard JA. VASER‑assisted… Aesthet Surg J. 2007;27(6):594–604.
- Aly A, Pace D, Cram A. Brachioplasty in the patient with massive weight loss. Aesthet Surg J. 2006;26:76–84.
- Aly AS, Cram A. Brachioplasty. Body Contouring after Massive Weight Loss. St Louis: QMP; 2006. pp.303–33.
- Bellini E, et al. A Journey Through Liposuction and Liposculture: Review. Ann Med Surg. 2017;24:53–60.
- Borges AF. W‑plastic dermolipectomy… Ann Plast Surg. 1982;9:498–501.
- Bracaglia R, et al. “Kris‑knife” brachioplasty… Aesthetic Plast Surg. 2013;37:640–2.
- Chandawarkar RY, Lewis JM. Fish‑incision brachioplasty. JPRAS. 2006;59:521–5.
- Correa‑Iturraspè M, Fernandez J. Dermatolipectomia braquial. Prensa Med Argent. 1954:2432.
- de Souza Pinto EB, et al. Brachioplasty technique with the use of moulds. Plast Reconstr Surg. 2000;105:1854–60.
- Fantozzi F. Brachial lifting using the BTV technique. Eur J Plast Surg. 2014;37:95–102.
- Ferraro GA, et al. Modified Fish‑Incision Technique… Aesthetic Plast Surg. 2015.
- Fischer A, Fischer G. First surgical treatment for moulding body’s cellulite… Bull Int Acad Cosmet Surg. 1976;3:35.
- Franco T. Cirurgia Estética. Rio de Janeiro: Ateneu; 1977.
- Gilliland MD, Lyos AT. CAST liposuction: an alternative… Aesthetic Plast Surg. 1997;21:398–402.
- Goddio AS. A new technique for brachioplasty. Plast Reconstr Surg. 1989;84:85–91.
- Guerrero‑Santos J. Brachioplasty. Aesthetic Plast Surg. 1979;3:1–14.
- Hurwitz DJ, Holland SW. The L brachioplasty… Plast Reconstr Surg. 2006;117:403–11.
- Juri J, Juri C, Elias JC. Arm dermolipectomy with quadrangular flap and “T” closure. Plast Reconstr Surg. 1979;64:521–5.
- Knotts CD, Kortesis BG, Hunstad JP. Avulsion brachioplasty… Plast Reconstr Surg. 2014;133:283–8.
- Kornstein AN. SERI Surgical Scaffold as an Adjunct… PRS Global Open. 2014;2:e190.
- Lockwood T. Brachioplasty with SFS suspension. Plast Reconstr Surg. 1995;96:912–20.
- Marques B, et al. Dermolipectomia braquial. Rev Soc Bras Cir Est Reconst. 1996;11.
- O’Toole J, et al. The History of Body Contouring Surgery. Semin Plast Surg. 2006;20(1):5–8.
- Pitanguy I. Abdominal lipectomy. Clin Plast Surg. 1975;2:401–10.
- Pitanguy I. Dermolipectomy of the abdominal wall, thigh, buttocks and upper extremity. In: Converse JM, ed. Reconstructive Plastic Surgery. 2nd ed. WB Saunders; 1977:190–198.
- Posse P. Cirurgia Estética. Buenos Aires: Ateneu; 1943.
- Regnault P. Brachioplasty, axilloplasty, and pre‑axilloplasty. Aesthetic Plast Surg. 1983;7:31–6.
- Regnault P. Brachioplasty, axilloplasty and pre‑axilloplasty. In: Ely JF, ed. Transactions of the 7th Int’l Congress of PRS. São Paulo: Cartgraf; 1980.
- Sisti A, et al. Complications Associated With Brachioplasty: A Literature Review. 2018;88(4):393–402.
- Strauch B, Greenspun D, Levine J, Baum T. A technique of brachioplasty. Plast Reconstr Surg. 2004;113:1044–8.
- Thorek M. Aesthetic surgery of the pendulous breast, abdomen and arms in females. Illinois Med J. 1930;3:48–57.
![Traveling After Arm Lift Surgery [ A Complete Guide ]](https://bodycontouringsurgery.com.au/wp-content/uploads/2023/11/BCSC_travelling_after_brachioplasty_surgery_-featured_image-1-150x150.jpg)