Complications After Thighplasty in Post‑Weight‑Loss Patients
Thighplasty, also known as thigh lift surgery, is a surgical procedure designed to remove excess skin, excess fat, and excess soft tissue of the thighs following significant weight loss. This type of thigh lift (thighplasty) surgery is commonly performed in post‑bariatric patients where skin quality and skin elasticity have been significantly altered. In post‑bariatric and massive weight‑loss patients, the medial and inner thighs are common problem areas due to reduced skin elasticity, altered blood supply, and changes in the underlying soft tissue.

Within body contouring and plastic surgery, thighplasty is recognised as a major surgery of the lower body associated with a relatively high rate of risks and complications when compared with other body contouring procedures. This is well documented in the medical literature, particularly for medial thigh lift (thighplasty) techniques that require long incisions and extensive soft tissue mobilisation [1–3].
This article provides a clear, evidence‑based discussion of complications after thighplasty, including wound complications, poor wound healing, blood clots, and other serious complications, with a focus on post‑weight‑loss patients undergoing thigh lift (thighplasty) surgery.
Why Complications Are Common After Thighplasty
The thighs present unique anatomical challenges that directly influence surgical outcomes. In post‑weight‑loss patients, these challenges are more pronounced.
Key factors contributing to wound complications and delayed recovery include:
- Constant movement and friction across the incision site
- Higher bacterial colonisation of the groin and inner thigh
- Thin skin and compromised blood vessels within the medial thigh
- Reduced skin elasticity after major weight reduction
- Tension is placed on healed incisions during walking and sitting
Across large pooled studies, overall complication rates after medial thighplasty range from 42–46%, with most events classified as minor complications [1,2]. In a comprehensive review of 447 patients, Sisti et al. reported an overall complication rate of 42.7% [1]. These figures highlight why prolonged follow up appointments and careful wound monitoring are routine after thighplasty.
Common Complications After Thighplasty Surgery
Most patients experience some form of wound‑related issue during the healing process. While these complications are often manageable, they can extend recovery and require ongoing care.
Wound Dehiscence and Wound Breakdown

Wound Breakdown
Wound dehiscence is the most frequently reported complication following thighplasty. Published studies report rates between 18.3% and 24%, particularly after medial and vertical thighplasty techniques [1–4].
Contributing factors include:
- High tension across the incision site
- Poor blood supply to medial thigh skin
- Reduced healing capacity after significant weight loss
- Smoking, nutritional deficiencies, or other underlying health conditions
Management typically involves local wound care, dressing changes, elastic bandage support, compression garment use, and close monitoring of wound healing at the surgical site. In selected cases, further surgery such as delayed surgical excision and closure may be considered once inflammation has settled. Delayed wound healing of 6–8 weeks is common and should be anticipated.
Seroma and Lymphatic Fluid Collections

Thigh seroma
Seroma formation is another common wound complication following thighplasty. Reported rates range from 8–25%, depending on the extent of dissection and surgical technique [1,4,5].
Seromas occur due to disruption of lymphatic channels, underlying tissue planes, and dead space within the soft tissue and skin fat layers. Pooled analyses suggest average rates around 8%, increasing to over 20% in extensive vertical medial thighplasty.
Management of seroma‑related wound complications may include:
- Needle aspiration
- Compression garment use
- Temporary placement of a thin tube or drain
- Rarely, surgical excision of the seroma cavity
Infection
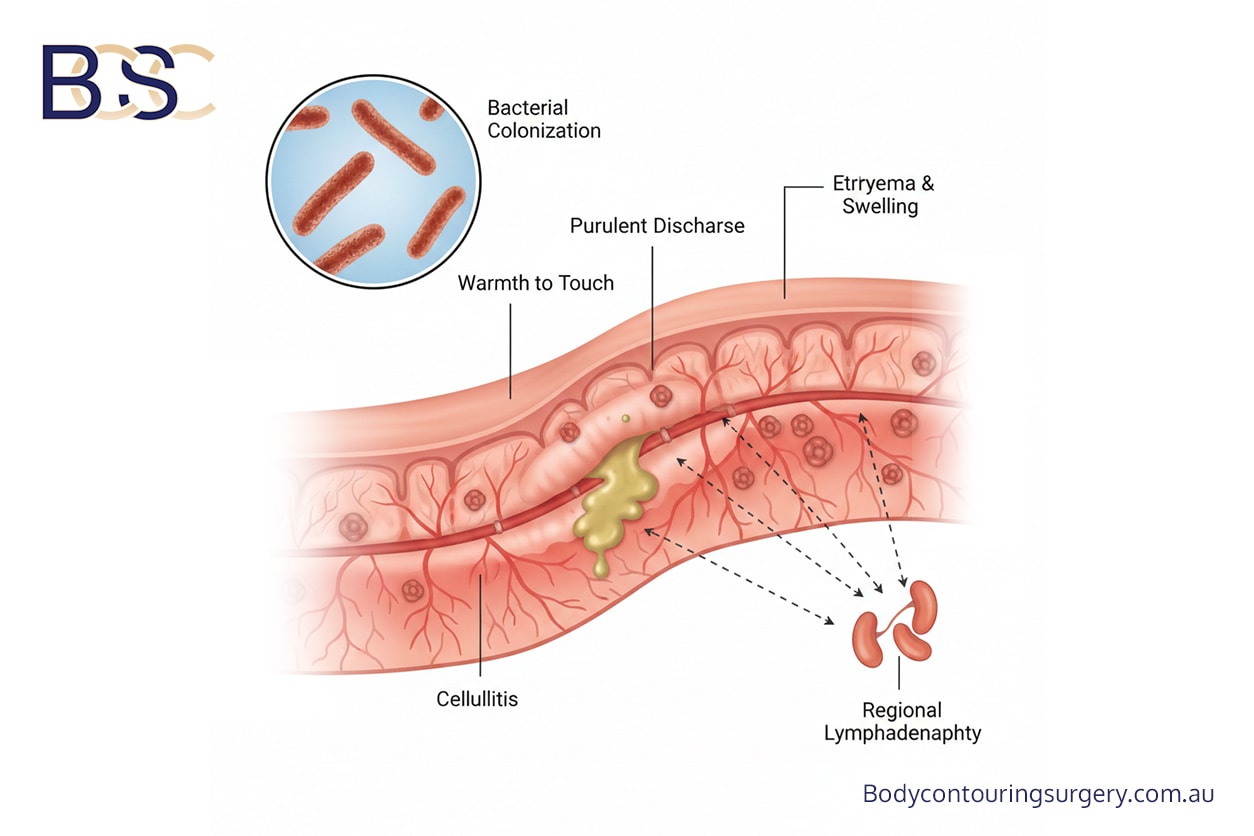
Post‑operative infection occurs in approximately 3–9% of thighplasty surgery cases, making infection one of the more common complications following this surgical procedure. Large retrospective studies report infection rates between 4.9% and 5.7% [1,4,6].
Infections usually involve the surgical site and may present with redness, warmth, discharge, or systemic symptoms. Treatment ranges from oral antibiotics and local wound care to hospital admission for intravenous therapy in more severe cases. Prompt medical attention is important to prevent progression.
Poor and Delayed Wound Healing
Poor wound healing and delayed wound healing are frequently encountered in post‑weight‑loss patients undergoing thighplasty. Contributing factors include reduced skin elasticity, compromised blood circulation, nutritional deficiencies, and medical comorbidities.
Management focuses on optimising nutrition, smoking cessation, consistent use of a compression garment, and extended post-operative care to support the healing process and reduce the risk of poor wound healing. Slow healing does not necessarily indicate surgical failure but reflects the altered healing physiology of massive weight‑loss patients.
Swollen Ankles and Lower Limb Swelling

Swollen lower leg
Swelling of the ankles and lower legs is a common complication after thighplasty, particularly following medial and vertical thighplasty techniques involving the inner thigh and medial thigh. Clinical series and post‑operative follow-up indicate that at least 10% of patients experience ankle or lower limb swelling.
This swelling is related to the temporary disruption of venous and lymphatic drainage. In some patients, swelling may persist for up to 12 months before gradually resolving. While concerning, this differs from true lymphoedema in most cases.
Supportive management includes:
- Ongoing use of compression garments
- Limb elevation
- Gradual return to activity
- Lymphatic drainage massage, which may assist lymphatic flow
Sudden swelling, chest pain, or shortness of breath requires immediate medical attention to exclude blood clots, deep vein thrombosis, or pulmonary embolism.
Scarring and Scar‑Related Issues

Hypertrophic scars
All thighplasty procedures result in permanent scars, and some patients may develop visible scars or hypertrophic scars depending on skin quality and healing response. Surgeons aim to limit scar length, but removal of large volumes of excess skin often necessitates longer incisions along the medial thigh or inner thigh.
Scar‑related issues may include widening, migration, hypertrophic scarring, or asymmetry. Scar maturation typically occurs over 12–18 months, and revision may occasionally be required.
Less Common but Serious Complications
Although less frequent, serious complications can occur and require careful counselling prior to surgery.
Blood Clots, Deep Vein Thrombosis, and Pulmonary Embolism

Blood clots
Blood clots are uncommon but potentially life‑threatening and represent one of the more serious complications associated with thigh lift (thighplasty) surgery and other modern surgery of the lower body. Reported rates of deep vein thrombosis and pulmonary embolism after thighplasty are approximately 0.1% [2,7]. Symptoms such as chest pain, shortness of breath, or painful leg swelling require immediate medical attention.
Lymphoedema
True lymphoedema is considered a rare but serious complication after medial thighplasty. Most swelling resolves over time, but persistent symptoms may occur, particularly in patients with pre‑existing lymphatic or vascular compromise.
Skin Necrosis
Partial skin loss due to compromised blood supply occurs in less than 1% of cases, with reported rates between 0.2–0.5% [1,4]. Management may involve prolonged wound care and, in selected cases, further surgery.
Factors Increasing Complication Risk

Scale
Recognised risk factors include:
- Massive or significant weight loss
- High or residual BMI
- Smoking
- Nutritional deficiencies
- Combined procedures such as body lift (belt lipectomy) surgery
- Long vertical incisions and extensive soft tissue undermining
A thorough review of the patient’s complete medical history, all the medications being taken, underlying health conditions, and overall physical health is essential prior to thigh lift (thighplasty) surgery.
Liposuction (suction-assisted lipectomy) and Complication Reduction

When carefully planned, liposuction may assist in removing excess fat deposits, reducing excess fat, and lowering excessive tension on the incision site, which may support wound healing and reduce delayed recovery. Evidence suggests that liposuction‑assisted thighplasty may reduce certain wound complications when used appropriately, though excessive liposuction may worsen poor wound healing.
Summary
Thighplasty after significant weight loss is a complex body contouring procedure with a well‑documented complication profile. While most complications are minor and manageable, prolonged wound healing, swelling, and the need for extended follow-up appointments are common.
Careful patient selection, realistic expectations, and structured postoperative care are critical to achieving surgical outcomes and recovery following thigh lift (thighplasty) surgery.
- Sisti A, Cuomo R, Zerini I, et al. Complications associated with medial thigh lift: a comprehensive literature review. J Cutan Aesthet Surg. 2015;8(4):191–197.
- Fischer JP, Wes AM, Serletti JM, Kovach SJ. Complications in body contouring procedures: an analysis of 1797 patients. Plast Reconstr Surg. 2013;132(6):1411–1420.
- Gusenoff JA, Coon D, Nayar H, et al. Medial thigh lift in the massive weight loss population: outcomes and complications. Plast Reconstr Surg. 2015;135(1):98–106.
- Michaels J, Coon D, Rubin JP. Vertical medial thigh contouring. Clin Plast Surg. 2019;46(1):91–103.
- Bertheuil N, Thienot S, Huguier V, et al. Medial thighplasty after massive weight loss: risk factors for postoperative complications. Aesthetic Plast Surg. 2014;38:63–68.
- Labardi L, Gentile P, Gigliotti S, et al. Medial thighplasty: horizontal and vertical procedures after massive weight loss. J Cutan Aesthet Surg. 2012;5:20–25.
- Hatef DA, Kenkel JM, Nguyen MQ, et al. Thromboembolic risk assessment in excisional body contouring surgery. Plast Reconstr Surg. 2008;122:269–279.

Location of practice: 30 Belmore Rd, Lorn, NSW 2320
Area of interest:
Body contouring surgery post pregnancy and post-weight loss, including Abdominoplasty, Mastopexy, Breast augmentation (Augmentation mammoplasty), Brachioplasty and Thighplasty.