Upper Arm Anatomy for Brachioplasty Patients
Brachioplasty surgery can lead to complications if the surgeon damages the underlying structures. Human arm anatomy consists of skin, fat, muscles, bones, nerves, and blood vessels. The soft tissues contribute to skin firmness or laxity, the latter of which is a common issue for patients seeking brachioplasty after weight loss or ageing.
Skin
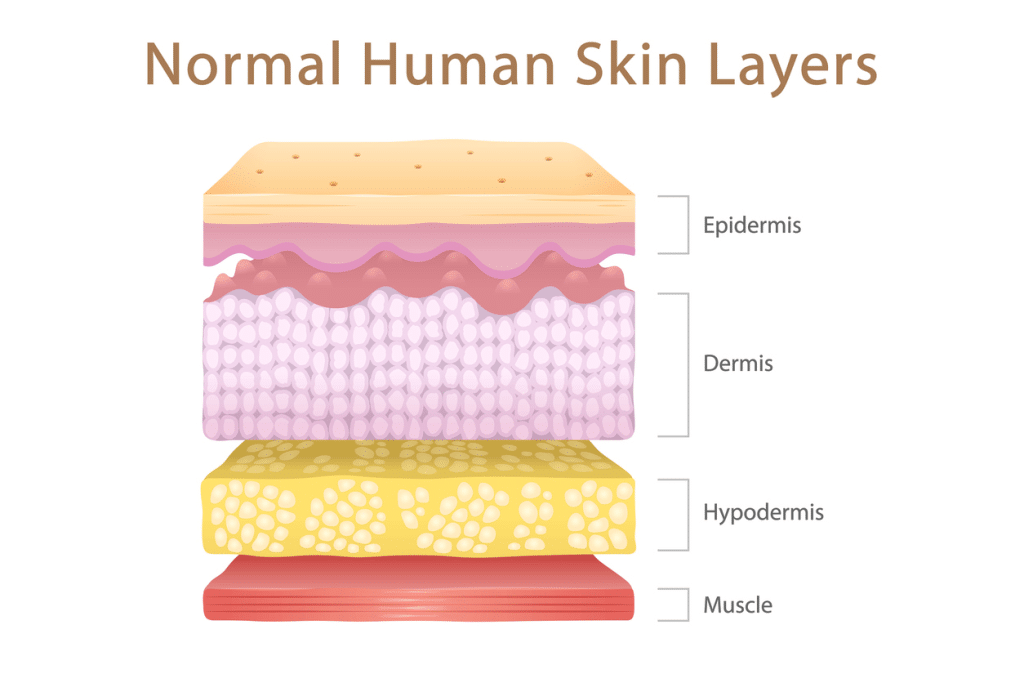
The skin is divided into three layers:
- Epidermis: The outermost skin layer
- Dermis: The middle layer where collagen and elastin are produced
- Hypodermis: The deepest layer of the skin is the subcutaneous fat layer
Arm Skin
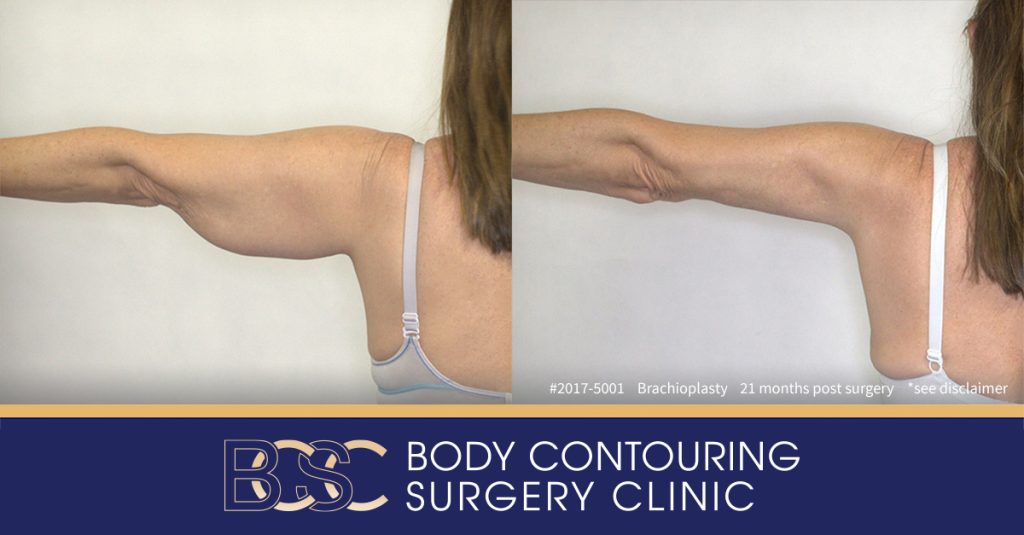
Disclaimer: Operation performed by Dr Bernard Beldholm. Adult content, surgery has risks; individual results vary, seek 2nd opinion. Please see the full disclaimer.
Skin firmness can be affected by ageing, genetics, diet, and sun exposure. Extreme weight gain can also damage the skin by stretching it beyond its limits.
Brachioplasty surgery tightens arms by trimming off the loose skin. As the incision is closed, the upper arms become slimmer and tighter.
Excess Arm Fat
Many people store excess fat in the upper limbs. Genetics, ageing, hormonal imbalances, dietary habits, and an inactive lifestyle play a role in how much arm fat a person has. Exercise and dieting are sometimes not enough to reduce arm fat. If the patient reaches a healthy weight and still has superficial fat deposits on the upper arms, liposuction (Suction assisted lipecotmy) may be appropriate. Liposuction can be performed on its own, although it often accompanies body contouring procedures such as brachioplasty surgery.
Brachioplasty also removes some fat in the hypodermis skin layer.
Bones
The skeletal structures of the upper limb consist of bones, cartilage, joints, and connective tissue. The musculoskeletal system also includes ligaments and tendons, such as the biceps tendon.
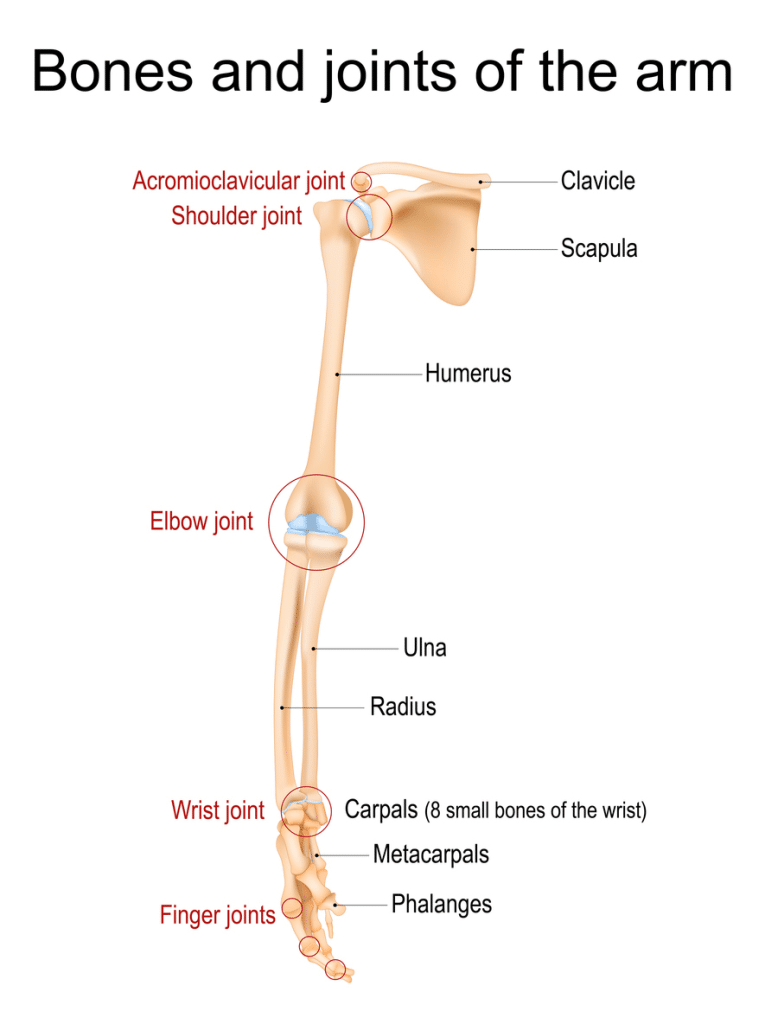
Bones in the upper extremity include the:
- Phalanges: These 14 bones make up the fingers.
- Metacarpal bones: These five small bones form the palm.
- Carpal bones: These eight small bones make up the wrist.
- Ulna: This forearm bone runs from elbow to wrist, on the same side as the pinky finger.
- Radius: This forearm bone runs parallel to the ulna, terminating at the wrist closest to the thumb.
- Scapula: The shoulder blade is a triangle-shaped bone that connects the humerus and the collarbone.
- Clavicle: The clavicle (collarbone) is a long, thin, horizontal bone above the ribcage that connects the sternum (breastbone) and shoulder.
- Humerus: The humerus (upper arm bone) sits between the shoulder bone and elbow joint. It connects to many muscles and ligaments throughout the entire upper limb.
The shoulder joint consists of the following:
- Glenohumeral joint: Connects the shoulder bone and humerus
- Sternoclavicular joint: Connects the collarbone and breastbone
- Acromioclavicular joint: Connects the shoulder bone and collarbone
The elbow joint consists of the:
- Proximal radioulnar joint: Moves the two forearm bones
- Radiohumeral joint: Moves the humerus and radius (lateral forearm bone)
- Ulnohumeral joint: Moves the humerus and ulna (the bone on the medial side of the forearm)
Arm Nerves
Surgeons must avoid damaging nerves in the upper extremity when performing brachioplasty surgery.
Brachial Plexus Nerves
The brachial plexus is a group of nerves that affect skin and muscle sensation in the shoulders, upper arm, forearm, and hands. These nerve roots originate at the spine and run down the length of the arm. The cubital fossa is the pathway for nerves that run along the upper arm to the forearm. If these nerves are damaged during an brachioplasty, it can affect cutaneous innervation and restrict muscle movement.
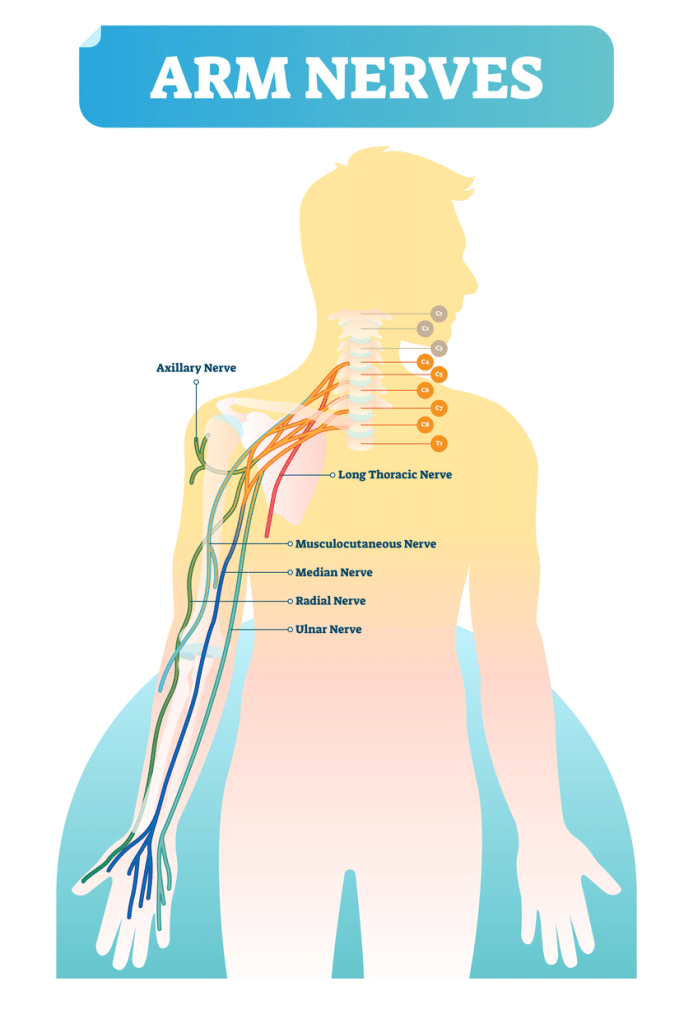
These five peripheral nerves are part of the brachial plexus
- Axillary nerve: Travelling between the shoulder and humerus, the axillary nerve stimulates the shoulder and part of the triceps brachii muscle.
- Ulnar nerve: The ulnar nerve, located on the outer forearm, stimulates the hand muscles and provides sensation to the pinky and part of the ring finger.
- Median nerve: The median nerve, located on the inner arm, activates the muscles in the wrist, hand, and forearm. It provides sensation to all the fingers (except the pinky).
- Musculocutaneous nerve: The musculocutaneous nerve, located in front of the humerus (upper arm bone), controls movement of the biceps, brachialis, and coracobrachialis muscles. It also provides sensation to the outer forearm.
- Radial nerve: The radial nerve stimulates the upper arm, wrist, and hand muscles. It also provides sensation to the thumbs. If the radial nerve is injured close to the armpit during brachioplasty surgery, the posterior compartment muscles (including the triceps muscle) won’t work properly.
Blood Vessels
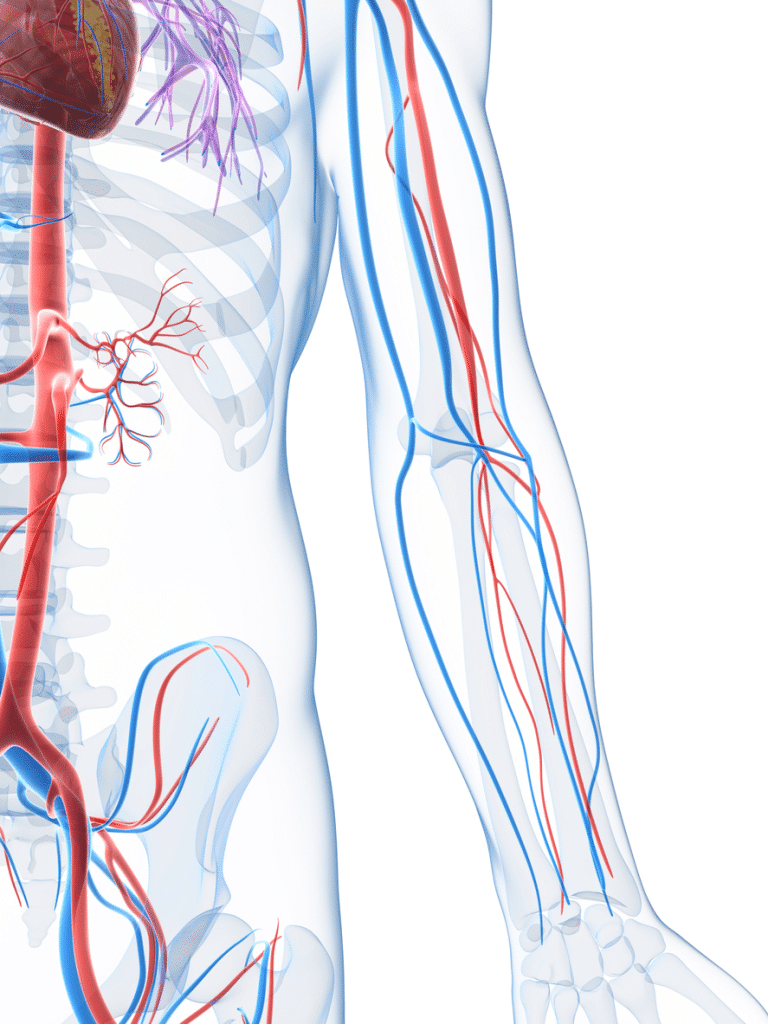
The upper limb contains several veins and arteries. Surgeons must take precautions to avoid damaging these structures duringbrachioplasty surgery. Otherwise, it can compromise the blood supply.
Some of the main blood vessels in the upper limb include the brachial artery, brachial veins, ulnar artery, ulnar veins, axillary artery, axillary vein, subclavian artery, cephalic vein, and basilic vein. The cubital fossa is a tiny, fat-filled depression in front of the elbow joint that acts as a passageway for the blood vessels between the forearm and upper limb.
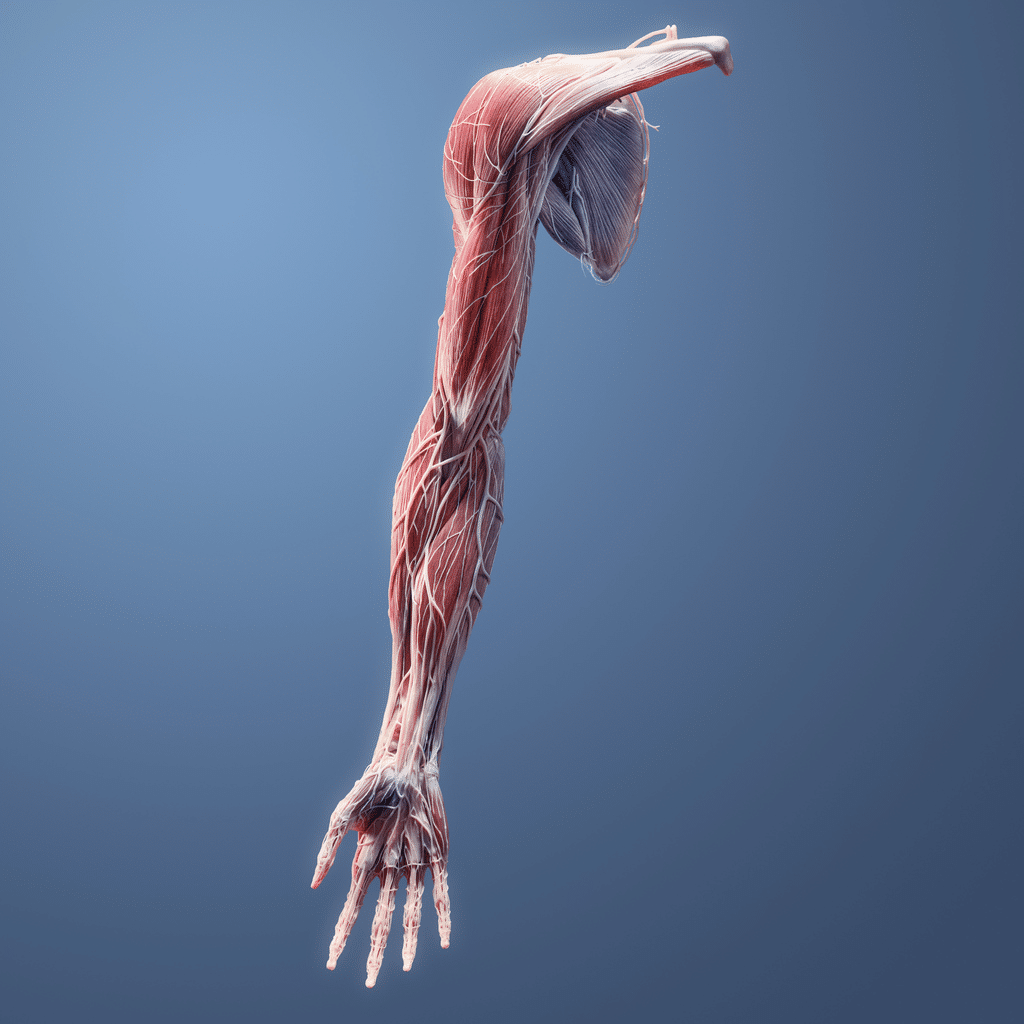
Arm Muscles
The upper limb has a complex system of muscles that work together to move the shoulders, arms, wrist, hand, and fingers. While it’s rare for muscle damage to occur during brachioplasty surgery, it’s possible if the surgeon lacks comprehensive knowledge of the arm anatomy.
Anterior and Posterior Division of the Upper Arm
The upper extremity is divided into two compartments, located on the front and back of the upper arm.
Anterior Compartment
There are three upper arm muscles in front of the humerus. The three muscles of the anterior compartment are the:
- Coracobrachialis. Located near the shoulder, the coracobrachialis adducts the upper arm and flexes the shoulder. It also stabilises the humerus where it meets the shoulder joint.
- Brachialis: The brachialis muscle is located beneath the biceps. The brachialis muscles bridge the upper arm bone and ulna bone in the forearm. The brachialis helps to flex the forearm.
- Biceps: The biceps brachii is one of the most superficial muscles in the upper extremity. It runs from the shoulder to the elbow. At the top, it divides into two muscular branches connecting to the front and back of the shoulder. The upper portion of the biceps brachii allows the upper arm to flex and adduct, while the lower part of the biceps brachii allows the forearm to flex toward the upper arm.
Posterior Compartment
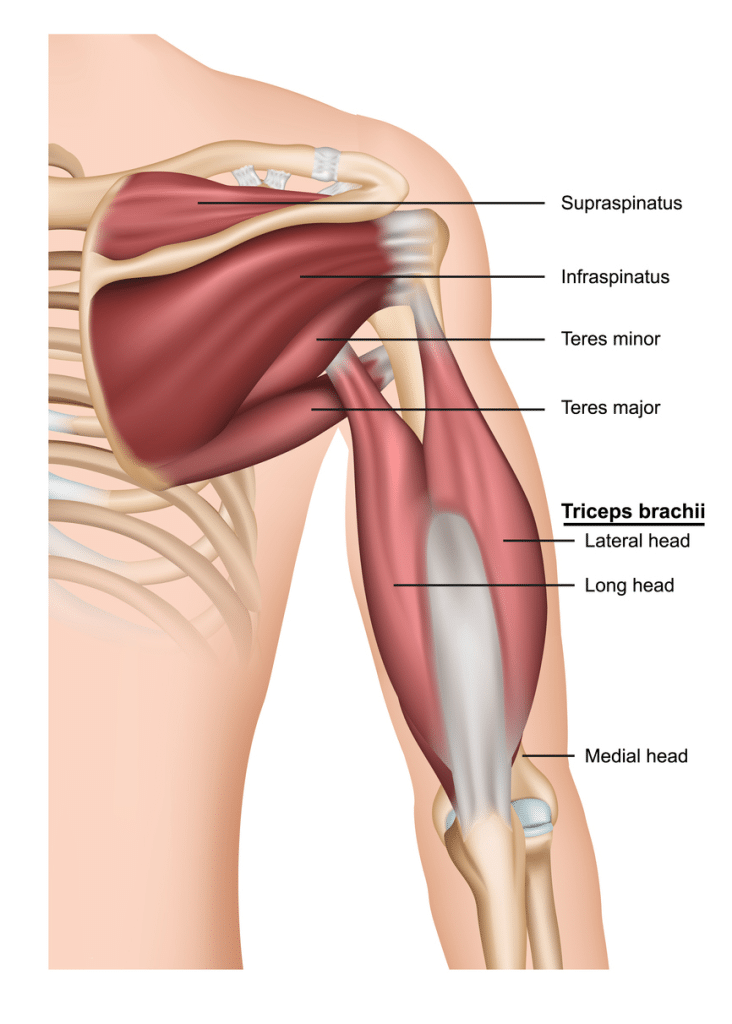
The posterior surface, or posterior compartment, is just behind the upper arm bone. The two muscles located in the posterior compartment are the:
- Anconeus: This small, triangular muscle aids in extending the elbow and rotating the forearm.
- Triceps Brachii: The triceps brachii muscle runs along the back of the upper arm bone. The lateral head of the tricep brachii muscle flexes and extends the forearm at the elbow joint. The triceps brachii also assists in stabilising the shoulder joint.
Forearm Muscles
The muscles on the anterior surface, or anterior compartment of the forearm, include the:
- Pronator teres: Rotates the forearm
- Palmaris longus: Helps flex the wrist
- Flexor pollicis longus: Flexes the thumb
- Extensor digiti minimi: Extends the pinky
- Pronator quadratura: Rotates the forearm
- Flexor carpi ulnaris: Allows for wrist flexion and adduction
- Flexor digitorum profundus: Aids in flexing the fingers and moving the wrist
- Flexor digitorum superficialis: Flexes the index, middle, ring, and pinky fingers
- Flexor carpi radialis: Flexes the wrist and aids in adduction of the hand and wrist
Like the upper arm, the forearm also has a posterior compartment. The muscles in the forearms’ posterior compartment are the:
- Supinator: Rotates the forearm
- Extensor carpi ulnari: Adducts the wrist
- Extensor indices: Extends the index finger
- Abductor pollicis longus: Abducts the thumb
- Extensor pollicis brevis: Extends the thumb
- Extensor carpi ulnaris: Extend and adducts the wrist
- Extensor pollicis longus: Extends the tip of the thumb
- Brachioradialis: Flexes the forearm closest to the elbow
- Extensor carpi radialis brevis: Extends and abducts the wrist
- Extensor digitorum: Helps extend all fingers, except the thumb
- Extensor carpi radialis longus: Abducts and extends the hand closest to the wrist joint
Clinical Significance for Brachioplasty Patients
Patients considering arm lift surgery (brachioplasty) are mainly interested in tightening skin and removing excess fat. An brachioplasty won’t correct vascular issues, nerve problems, poorly toned muscles, or bone deformities.
Arm anatomy is complex. When performing brachioplasty surgery, surgeons must be careful not to damage underlying structures such as the nerves, veins, and musculoskeletal system. This can lead to complications like nerve damage, excessive pain, or uncontrolled bleeding for the patient.
Brachioplasty patients should choose an experienced surgeon with extensive knowledge of upper limb anatomy and body contouring procedures.
