Diastasis of the rectus abdominis muscles (DRAM) is a condition in which the two vertical abdominal muscles, commonly called the “six-pack muscles,” separate due to overstretching of the connective tissue between them. This connective tissue is called the linea alba.
Clinically, diastasis recti is defined as an inter-rectus distance (IRD) of more than 30 mm, three centimetres above the umbilicus (belly button), measured at rest. While a small separation can be normal, larger gaps may cause both cosmetic and functional issues.
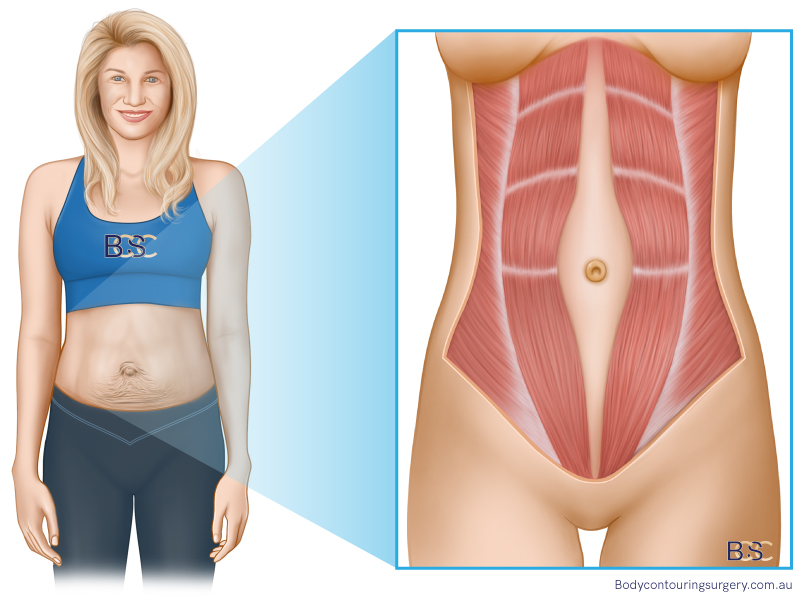
Understanding the Anatomy
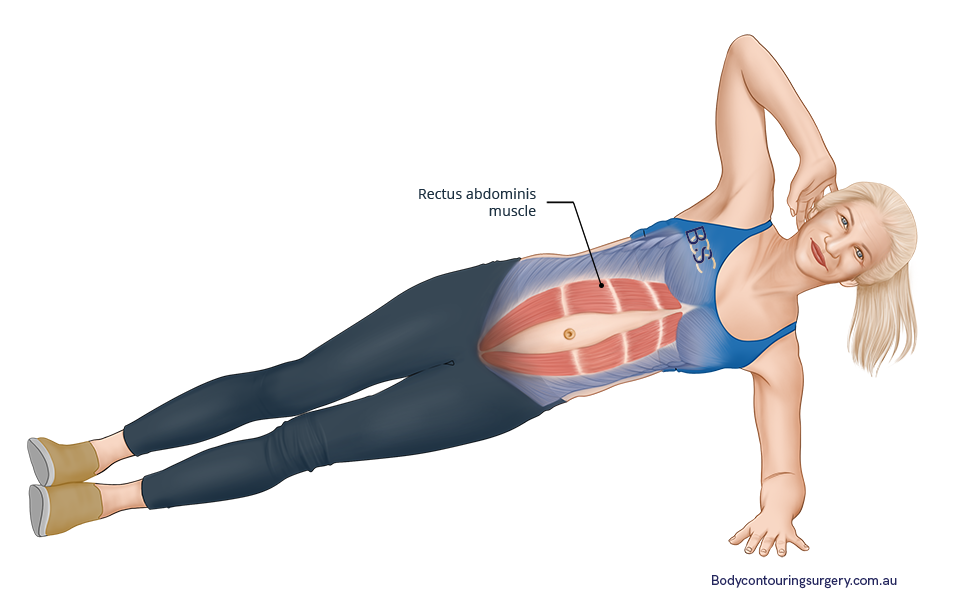
The rectus abdominis muscles run vertically from the rib cage to the pubic bone. The linea alba is the fibrous midline tissue that joins these muscles.
The linea alba naturally stretches during pregnancy and periods of weight gain. If overstretched, it can lose elasticity and remain widened, leading to muscle separation.
Alternate Names for Diastasis Recti
This condition may be described using several terms, including:
- Diastasis recti abdominis
- Rectus diastasis
- Rectus divarication
- Abdominal separation
- Split abdominal muscles (colloquial)
Causes of Diastasis Recti
Pregnancy
Pregnancy is the most common cause of DRAM. The growing uterus places pressure on the abdominal wall, especially in the second and third trimesters. Research suggests that up to two-thirds of pregnant women develop some degree of separation (diastasis recti).
Risk Factors During Pregnancy
Certain factors increase the likelihood of experiencing DRAM:
- Multiple pregnancies, especially spaced closely together
- Maternal age over 35 years
- Carrying twins, triplets, or a large baby
- Vaginal delivery
- Petite or slightly built body type
- Intense abdominal exertion during pregnancy
Infants
Newborns can sometimes show a visible midline separation because their abdominal wall has not fully developed. This usually resolves on its own within the first two years of life.
Men and Non-Pregnant Women
Diastasis recti can also occur in men and women unrelated to pregnancy. Significant weight gain, obesity, or repetitive heavy lifting may stretch the linea alba and lead to separation.
Symptoms of Diastasis Recti
Diastasis recti can affect both function and appearance. Some patients notice changes in abdominal shape, while others experience discomfort or secondary problems.
Abdominal Separation or Dome-Shaped Appearance
When contracting the abdominal muscles, such as during a sit-up, the midline may project outward in a ridge-like or dome-shaped fashion instead of flattening. This occurs because the rectus abdominis muscles are no longer held together effectively.
Soft or Less Firm Midsection
Around the umbilicus, the abdominal wall may feel softer or less stable. This results from thinning of the linea alba, which reduces support in the midline.
Core Muscle Weakness
The separation reduces core stability, making it harder to sit up, maintain posture, or perform activities that require trunk strength. Patients may experience fatigue or weakness with daily tasks.
Lower Back Discomfort
With reduced abdominal support, the back muscles must compensate to maintain posture. Over time, this can cause muscular strain and persistent lower back discomfort.
Urinary Incontinence
A weakened abdominal wall places extra demand on the pelvic floor. Some patients develop persistent bladder leakage, particularly when coughing, sneezing, laughing, or exercising.
Digestive Concerns
Gastrointestinal symptoms such as bloating, constipation, or abdominal discomfort are sometimes reported. A 2021 systematic review also identified abdominal pain as a common self-reported symptom among women with diastasis recti.
Development of a Hernia
Significant abdominal separation may increase the likelihood of a hernia, where internal tissue pushes forward through the weakened midline. Hernias may require surgical repair.
Pelvic Organ Prolapse
Since the abdominal wall and pelvic floor function together, weakness in both can contribute to pelvic organ prolapse. This occurs when organs such as the bladder, uterus, or rectum shift downward from their usual position, sometimes creating a sensation of pelvic heaviness.
Postural Changes
Patients often adapt by leaning backward or slouching forward, leading to poor posture. These changes can worsen discomfort in the lower back and hips.
Difficulty with Exercise and Everyday Activities
Daily tasks such as lifting children, carrying shopping bags, or returning to exercise may feel more difficult. The abdominal wall may not activate effectively, making some movements uncomfortable or unsafe.
How to Diagnose Diastasis Recti
Self-Examination at Home
A simple home check involves:
- Lying on your back with knees bent and feet flat.
- Placing one hand behind your head and the other across your abdomen.
- Slowly lifting your head and shoulders.
- Feeling along the midline for separation with your fingers.
- A gap greater than one finger’s width may indicate diastasis recti.
Clinical Diagnosis
Diagnosis may be confirmed with:
- Physical examination by a qualified health professional
- Ultrasound imaging, the most reliable non-invasive method
- CT or MRI scans, if a detailed evaluation is required
Treatment Options for Diastasis Recti
Conservative Management
Mild cases often improve naturally in the months after pregnancy. Non-surgical options include:
- Physiotherapy programs, especially postpartum rehabilitation exercises
- Abdominal binders or support garments to temporarily assist the abdominal wall
- Lifestyle adjustments, such as maintaining a healthy weight and avoiding high-strain abdominal activity
Surgical Management
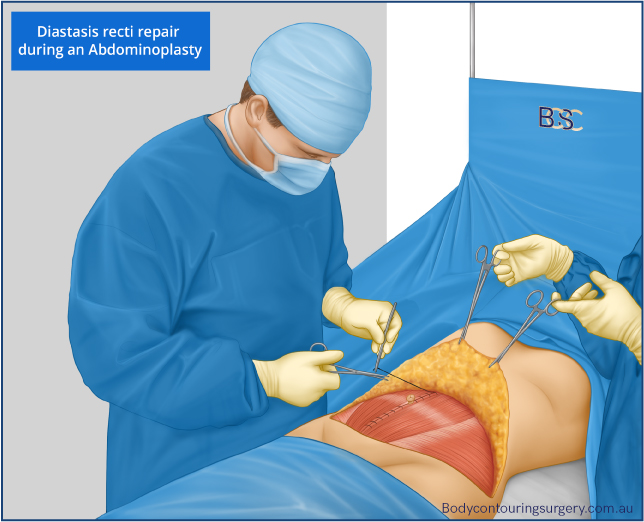
For persistent or severe separation, surgery may be considered. Abdominoplasty (tummy tuck surgery) involves:
- Repositioning the rectus abdominis muscles
- Reinforcing the linea alba with sutures
- Removing excess skin and fat, if present
Surgical repair can restore abdominal wall function but also carries risks, including scarring, wound complications, and recurrence after pregnancy. It is generally advised to delay surgery until childbearing is complete.
Medicare Support for Surgery
In July 2021, the Australian Government reinstated Medicare Item Number 30175 for eligible patients requiring abdominoplasty for DRAM after pregnancy.
Eligibility criteria include:
- At least 12 months postpartum
- A documented separation of 30 mm or more
- Ongoing functional symptoms such as pain, incontinence, or difficulty with daily activities despite supervised physiotherapy or exercise programs
Approval is subject to strict criteria and assessment by a specialist surgeon.
Living with and Overcoming Diastasis Recti
While diastasis recti is not life-threatening, it can significantly affect quality of life. Many patients adapt with conservative measures, while others require surgical correction for meaningful improvement.
Successful management can improve continence, reduce back discomfort, enhance posture, and restore abdominal stability. The right approach depends on individual symptoms, lifestyle goals, and medical suitability.
Sources
- Laura Fuentes Aparicio, Montserrat Rejano-Campo, Gráinne Marie Donnelly, Victoria Vicente-Campos (2021) “Self-reported symptoms in women with diastasis rectus abdominis: A systematic review” Journal of Gynecology Obstetrics and Human Reproduction, Volume 50, Issue 7, September 2021
Links
- mbsOnline.gov.au. March 29, 2022 “New MBS item 30175 for abdominoplasty” [Accessed June 23, 2023]
