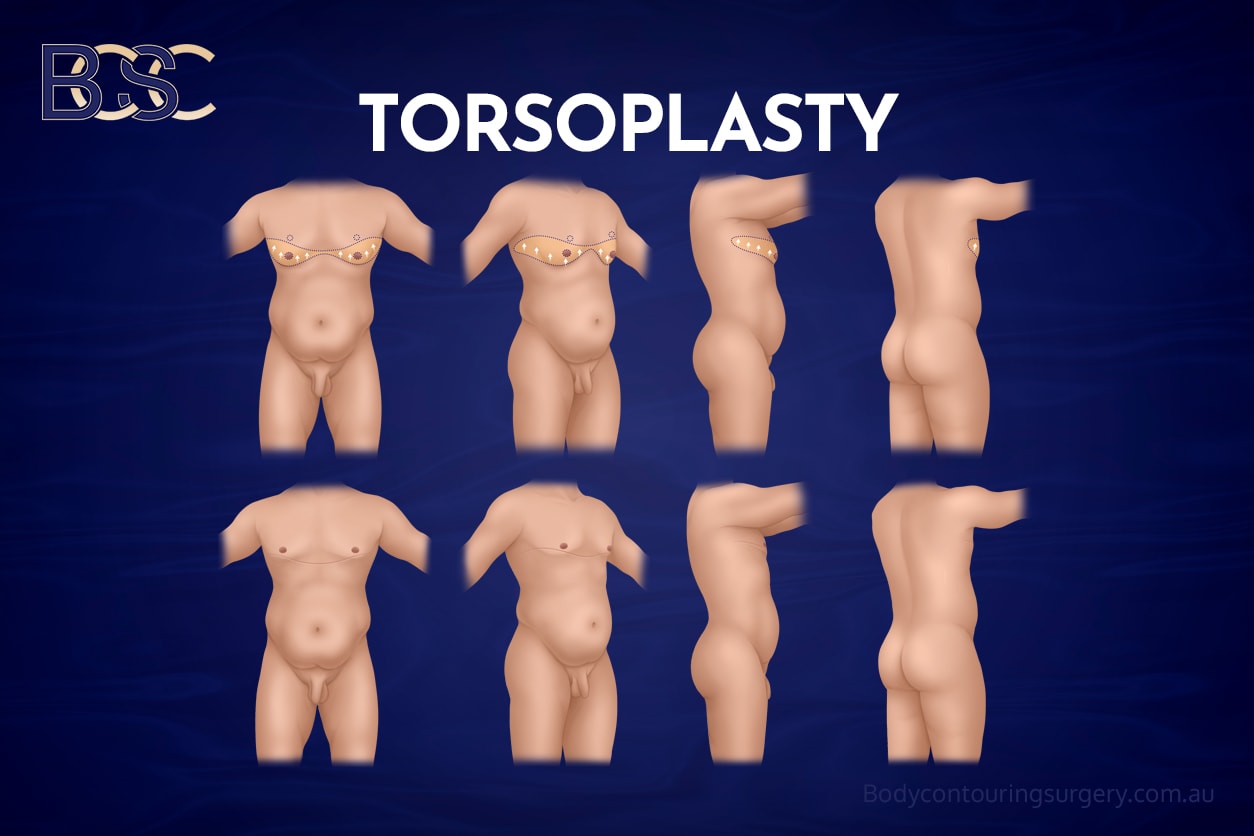
Upper Body Lift (Torsoplasty) Surgery for Men After Massive Weight Loss
Male chest surgery after major weight loss may be considered for men who have experienced significant changes in their bodies following weight reduction and continue to have physical concerns related to excess, lax, or residual skin and fat of the chest and upper body. While weight loss is associated with benefits for metabolic health and mobility, it does not consistently reverse the structural changes in the skin and soft tissues that occur during prolonged obesity.
After massive weight loss, some men notice that the chest and upper torso retain loose or hanging tissue that does not resolve with exercise or further weight reduction. This may contribute to large skin folds, ongoing skin irritation, hygiene difficulties, and functional concerns related to clothing or physical activity. Individual experiences vary, and not all patients will experience the same degree of concern.
An upper body lift (upper torsoplasty) is a reconstructive surgical procedure that may be used to treat excess skin of the upper torso following major weight loss. At Body Contouring Surgery Clinic (BCSC), upper torsoplasty is considered part of a structured, individualised approach to post–weight-loss body contouring in men. Surgical outcomes vary between individuals.
Why the Male Chest May Change After Significant Weight Loss

The Role of Skin Stretching and Elasticity Loss
Changes in the male chest following significant weight loss are influenced by a combination of skin quality, fat distribution, and, in some patients, the presence of gynaecomastia or pseudogynaecomastia prior to weight loss.
During periods of excess body weight, the skin stretches to accommodate increased fat volume. Over time, changes in collagen and elastin can reduce the skin’s ability to retract. When weight is lost, particularly following bariatric surgery or rapid weight loss, the underlying volume decreases, but the stretched skin may not fully contract.
The Influence of Gynaecomastia
In addition to skin changes, breast tissue characteristics play an important role. Gynaecomastia, which involves true glandular breast tissue, is a common complaint in male patients and may coexist with weight gain. In men with significant gynaecomastia, weight loss does not reliably reduce glandular volume.
Following weight loss, these patients may be left with a fuller, more ptotic breast that retains a noticeable amount of breast tissue. In some cases, this pattern of chest change requires more extensive surgical excision to address both volume and excess skin.
Pseudogynaecomastia and Weight-Related Breast Changes
By contrast, men who gain a significant amount of weight commonly develop pseudogynaecomastia, where breast enlargement is primarily related to excess fatty tissue rather than glandular tissue. This fatty enlargement stretches the skin over time.
When weight is lost, pseudogynaecomastia itself often resolves as fat volume reduces. However, the skin that was stretched during weight gain may remain lax. These patients may present with limited residual breast volume but significant loose skin.
Differences in Post–Weight Loss Chest Appearance

As a result, the post–weight loss appearance of the male chest can differ substantially:
- Men with underlying gynaecomastia may have persistent breast volume combined with skin laxity, leading to a fuller and more ptotic chest.
- Men with previous pseudogynaecomastia may have reduced volume after weight loss, but are often left with excess skin and poor chest definition.
Factors Contributing to Persistent Chest Changes
Factors that may contribute to persistent chest changes include:
- The total amount of weight loss
- Duration of obesity prior to weight loss
- Presence and severity of gynaecomastia or pseudogynaecomastia
- Age at the time of weight loss
- Genetic skin characteristics
- Smoking history
- Repeated or significant weight fluctuations
As a result, some men are left with excess skin & tissue, and visible skin folds across the chest and upper body, despite reaching a stable weight.
Common Upper Body Concerns After Massive Weight Loss
Men presenting after massive weight loss may report concerns such as:
- Excess skin affecting the chest
- Skin folds along the lower chest or bra line region
- Excess back skin extending toward the shoulder blade area
- Loose skin beneath the arms or in the upper arms
- Recurrent skin irritation or rashes within skin folds
- Discomfort during physical activity due to skin movement
- Ongoing difficulty with clothing fit or body image
These concerns may be functional & physical in nature and can vary in severity between individuals.
Gynaecomastia, Pseudogynaecomastia, and Post–Weight Loss Chest Changes
Post–weight loss chest changes differ from standard gynaecomastia.
- Gynaecomastia refers to the enlargement of glandular breast tissue.
- Pseudogynaecomastia describes enlargement related primarily to fatty tissue.
- Post–weight loss chest changes are commonly associated with excess skin, generalised skin laxity, and residual soft tissue following major weight reduction.
Management approaches differ between these conditions. Techniques used for isolated gynaecomastia may not adequately treat widespread skin laxity following significant weight loss, and treatment planning requires careful individual assessment.

Indications for Upper Body Lift (Upper Torsoplasty)
Upper body lift surgery (upper torsoplasty) is primarily indicated for men who experience significant loose skin of the upper chest and upper torso following massive weight loss. The key driver for surgery is skin excess rather than residual fat volume, and careful assessment is required to determine the pattern and extent of laxity.
In the chest, excess skin is commonly described as ptosis. In male patients, this may be defined as descent of the nipple–areola complex (NAC) below the lower border of the pectoralis major muscle, which functions as the male equivalent of the inframammary fold. In other cases, men may demonstrate pseudo-ptosis, where there is a significant amount of loose skin and residual volume within the breast envelope, even if the NAC position is relatively preserved.
Both ptosis and pseudo-ptosis can contribute to a poor chest appearance and are common indications for surgical excision following major weight loss.
Years of experience
24/7 support
Qualified doctors
Many specialties
Modern facilities
Guaranteed results
Pattern of Skin Laxity and Surgical Planning
The distribution of loose skin across the upper torso plays a central role in determining the appropriate surgical approach.
Anterior Chest Skin Laxity
When excess skin is predominantly located on the anterior chest, with minimal involvement of the lateral chest wall or upper back, an anterior upper torsoplasty may be considered. This approach focuses on excision of redundant skin across the chest and upper abdomen while limiting the extent of posterior scarring.
Anterior torsoplasty is commonly indicated in patients with chest ptosis or pseudo-ptosis, where skin excess is confined to the anterior torso.
Lateral Chest and Upper Back Skin Laxity
When loose skin extends beyond the anterior chest to involve the lateral chest wall and upper back, an upper circumferential torsoplasty may be indicated. In these patients, treating the chest alone may leave residual folds or contour imbalance.
Circumferential torsoplasty allows for excision of excess skin across the chest, bra line region, and upper back, providing a more balanced correction of the upper torso. Not all patients require circumferential treatment, and the decision is individualised.
Role of Liposuction in Post–Weight Loss Patients
In men following massive weight loss, liposuction is not always required as part of upper torsoplasty. Many patients have already lost substantial fat volume, and the primary issue is excess skin rather than excess fat.
In selected cases, liposuction (suction-assisted lipectomy) may be added as an adjunct to treat focal areas of residual fat or to refine contour. The decision to include liposuction is based on physical examination findings and is not routine for all post–weight loss patients.
Who May Be Considered for Upper Torsoplasty
Upper torsoplasty may be considered in patients who:
- Have maintained a stable weight for a period of time
- Are medically suitable for surgery
- Do not have uncontrolled medical conditions
- Experience physical or functional concerns related to excess upper body skin
- Have realistic expectations regarding surgery, recovery, and scarring
A comprehensive medical history, physical examination, and discussion of alternative management options are essential components of the consultation process.
The Surgical Procedure and Anaesthesia
Upper body lift surgery (upper torsoplasty) is performed under general anaesthesia. The procedure involves careful dissection through tissue layers while preserving blood supply and minimising trauma to surrounding structures.
The surgical approach is planned to balance tissue removal with wound healing. Individual operative details vary.
Hospital Stay and Early Postoperative Care
Patients typically remain in the hospital for one to two nights, depending on the extent of surgery and individual recovery. Pain management is provided using appropriate pain medications, and early gentle mobilisation is encouraged to reduce the risk of blood clots.
Surgical drains may be used temporarily to manage fluid accumulation.
Recovery Timeline and Activity Considerations
Recovery following upper torsoplasty varies between individuals and depends on the surgical extent. General timelines may include:
- First two weeks: swelling and activity modification
- Weeks three to four: gradual increase in daily activities
- Around four weeks: consideration of light exercise
- Six to eight weeks: Heavy lifting and strenuous activity may be commenced
Patients are provided with individualised postoperative instructions. A compression garment is recommended during recovery.
Wound Care, Scarring, and Follow-Up
Incision sites are reviewed during scheduled follow-up appointments to monitor wound healing. Once wounds have healed, silicone-based products may be considered for scar management.
Scarring is an expected outcome of surgery. Scar appearance and maturation vary between individuals and over time.

Risks and Complications
Upper torsoplasty is a major surgical procedure and carries recognised risks, which may include:
- Wound infection
- Delayed wound healing
- Seroma formation
- Blood clots
- Changes in skin or nipple sensation
A detailed discussion of risks, potential complications, and alternative options forms part of the informed consent process.
Long-Term Considerations
Some patients report physical comfort or ease of daily activities following upper torsoplasty; however, outcomes vary. Long-term results depend on factors such as weight stability, healing, and individual health.
Final Notes
An upper body lift (upper torsoplasty) is a reconstructive surgical option that may be considered for selected patients following massive weight loss. It is not suitable for everyone, and outcomes vary between individuals. This information is general in nature and does not replace consultation with a qualified medical practitioner.
Frequently Asked Questions
Torsoplasty refers to surgical procedures that remove excess skin and tissue from the torso (chest) following significant weight loss.
Recovery timelines vary. Initial recovery commonly spans several weeks, with ongoing changes over several months.
In cases where excess skin is present, surgical skin removal may be discussed as one management option following assessment.
Activity restrictions, including avoidance of heavy lifting and strenuous exercise, are commonly advised during early recovery. Individual guidance is provided by the treating surgeon.
Years of experience
24/7 support
Qualified doctors
Many specialties
Modern facilities
Guaranteed results
How to get started
Ask your GP for a referral, then book a consultation with Dr Beldholm. At your consultation, your suitability is assessed and your options, the risks and the recovery are explained.

