Preparation involves detailed consultation and planning. Nutritional assessment is particularly important in bariatric surgery patients, as vitamin or protein deficiencies increase risks of infection or delayed healing [2]. Smoking should be stopped at least four weeks before surgery [3]. Patients are advised to arrange home support for the recovery period and to attend at least two consultations before surgery [1].
The Operation
Abdominoplasty surgery is carried out under general anaesthetic in an accredited hospital. The procedure takes three to five hours. Patients usually stay in hospital for one to three days [4].
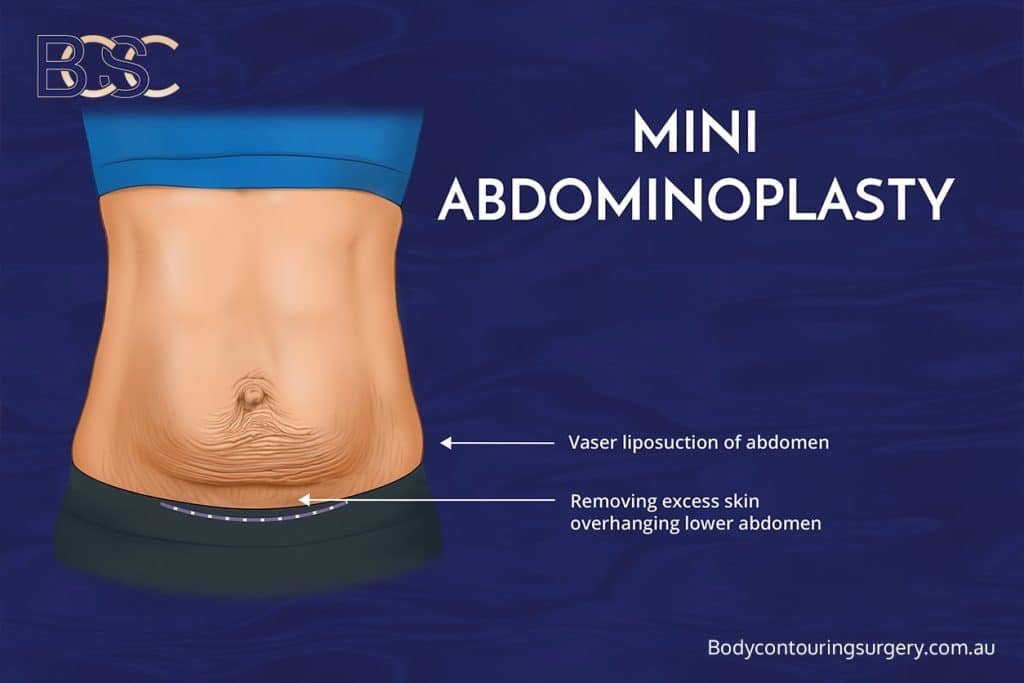
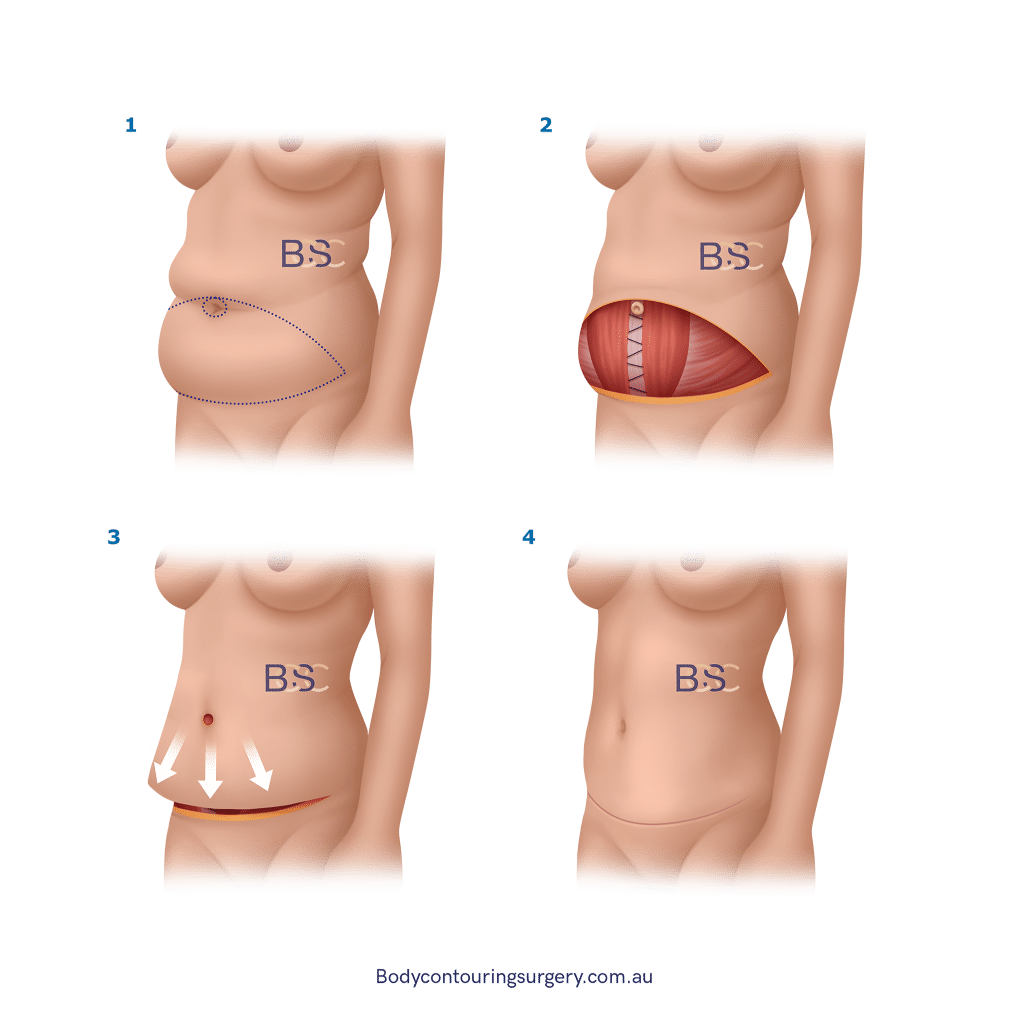
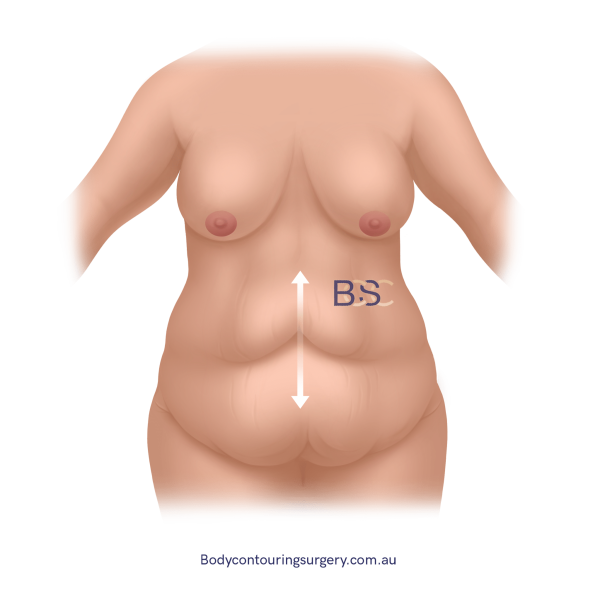
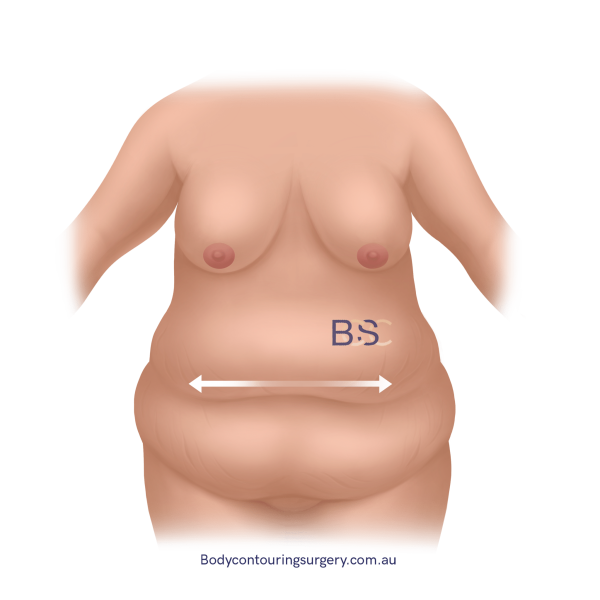
The surgeon makes a low abdominal incision, lifts skin and fat, repairs or tightens abdominal muscles (diastasis recti), and removes excess tissue. In most cases, the belly button is repositioned. Compression garments and drains may be used. Some patients undergo combined procedures such as suction assisted lipectomy [6].
Recovery and Aftercare
Recovery after tummy tuck (abdominoplasty) surgery is gradual. Early walking is encouraged to reduce the risk of blood clots such as deep vein thrombosis [5]. Compression garments help support healing [6].
Most patients can return to light work after two to three weeks. Gentle exercise may begin after six weeks, while strenuous activity is avoided for at least eight weeks. Scars usually mature over 12 to 18 months [3].
Risks and Potential Complications
Every surgical procedure has risks. Possible complications of abdominoplasty include bleeding, infection, seroma, haematoma, poor wound healing, pulmonary embolism, skin sensation changes, and scarring [4,5]. Published studies report rates of infection at 4%, wound separation at 8.6%, seroma at 8.4%, and haematoma at 2.6% [1].
Timing After Bariatric Surgery
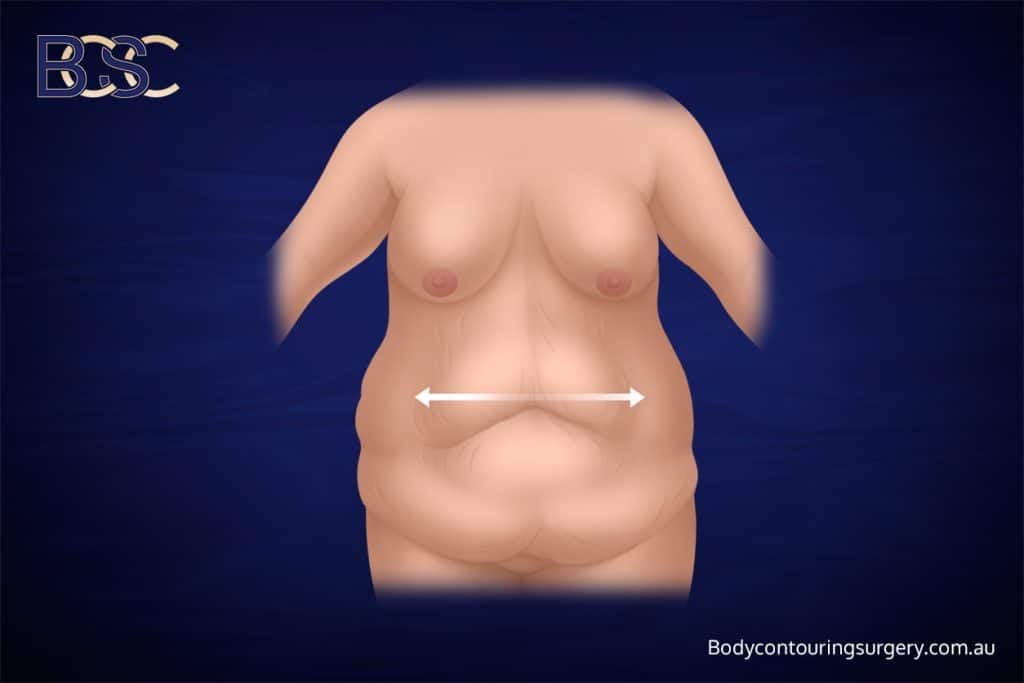
Most surgeons recommend waiting at least 12–18 months after bariatric surgery before undergoing abdominoplasty. This allows time for weight to stabilise and for nutritional recovery [2,6]. In cases of severe pannus-related infections, early panniculectomy may be considered [1].