Why the Thighs Commonly Develop Excess Skin After Weight Loss
The thighs have a large skin surface area in the lower body and are particularly prone to skin laxity after weight loss. During weight gain, the skin stretches to accommodate increased fat volume. After weight loss, particularly after bariatric surgery, the underlying fat reduces, but skin elasticity is often permanently compromised.
As a result, many patients experience:
- Excess skin along the inner thigh and medial thigh
- Circumferential skin excess around the upper thighs
- Skin folds extending toward the knee
- Areas of moisture, friction, and skin irritation
These issues frequently persist despite long‑term weight stability and a healthy diet. For many patients, thigh lift (thighplasty) surgery is part of a broader approach to post‑weight‑loss body-contouring procedures.
Understanding Medial Thigh Skin Laxity and Surgical Planning
A critical concept in medial thigh lift (thighplasty) surgery is the recognition that excess skin develops in multiple directions. In most post‑weight‑loss patients, loose skin affects the thighs both circumferentially and vertically. Failure to treat both components often leads to incomplete correction.
Circumferential Skin Excess
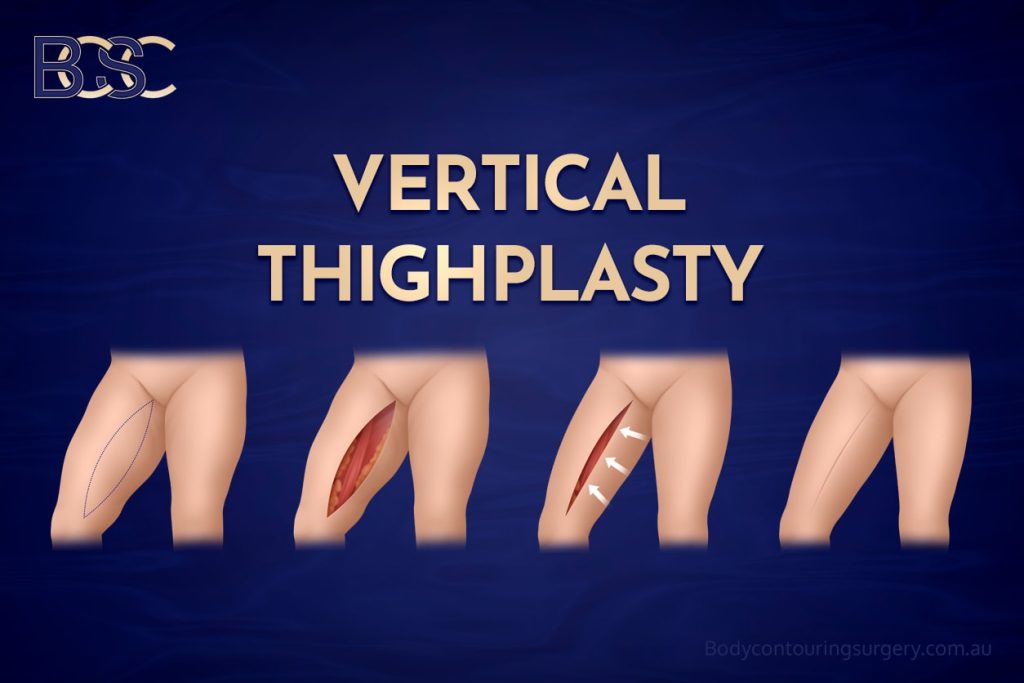
Circumferential excess skin increases the girth of the thighs and is best managed with a vertical incision along the medial thigh. This approach reduces thigh circumference but does not adequately lift hanging skin in the groin area.
Vertical (Hanging) Skin Excess
Vertical excess skin typically presents as hanging skin in the upper inner thigh and groin crease. This pattern requires a horizontal incision within the groin crease to elevate and support the skin.
Most patients who have experienced significant weight loss have both patterns of skin excess. For this reason, the procedure varies depending on anatomy, and a single‑direction thigh lift (thighplasty) often leaves residual loose skin.




 Skin Excess")

")