The Dual Vector Abdominoplasty Concept
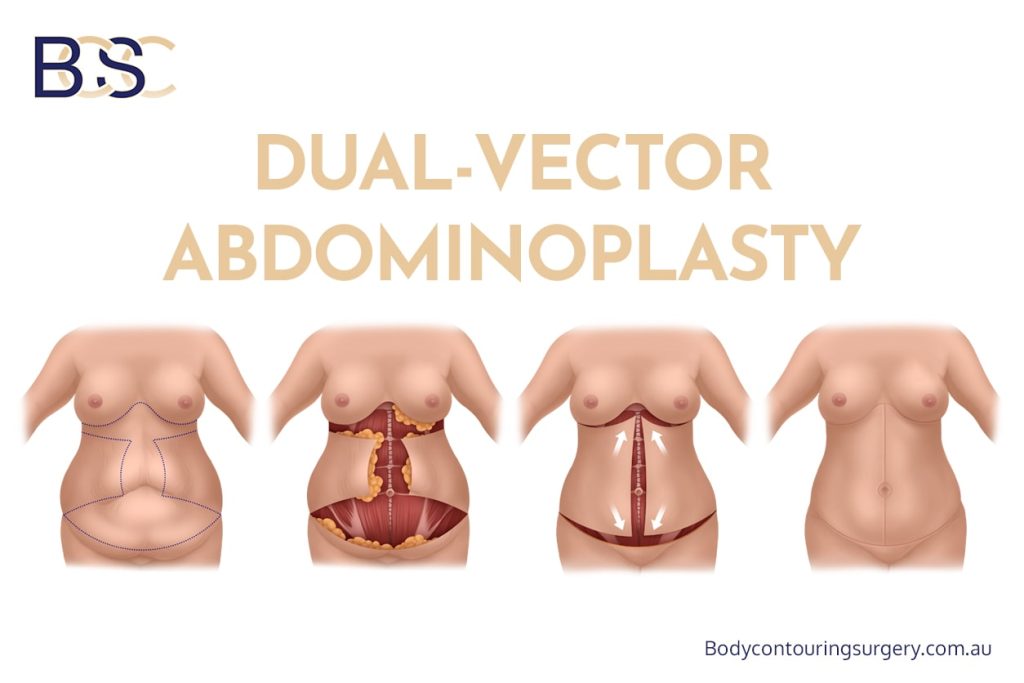
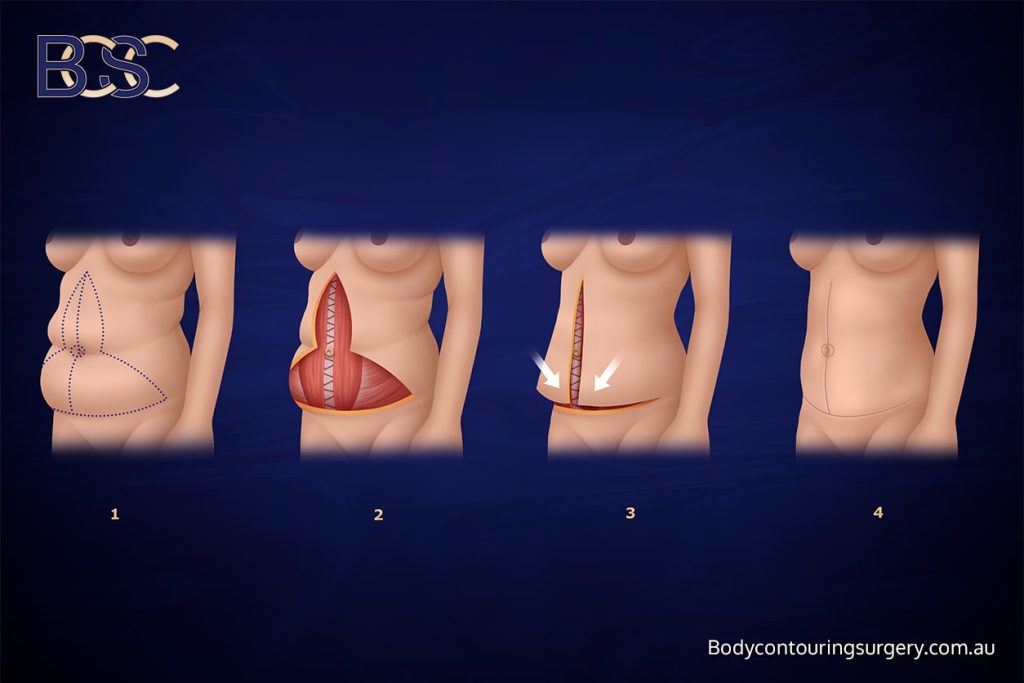
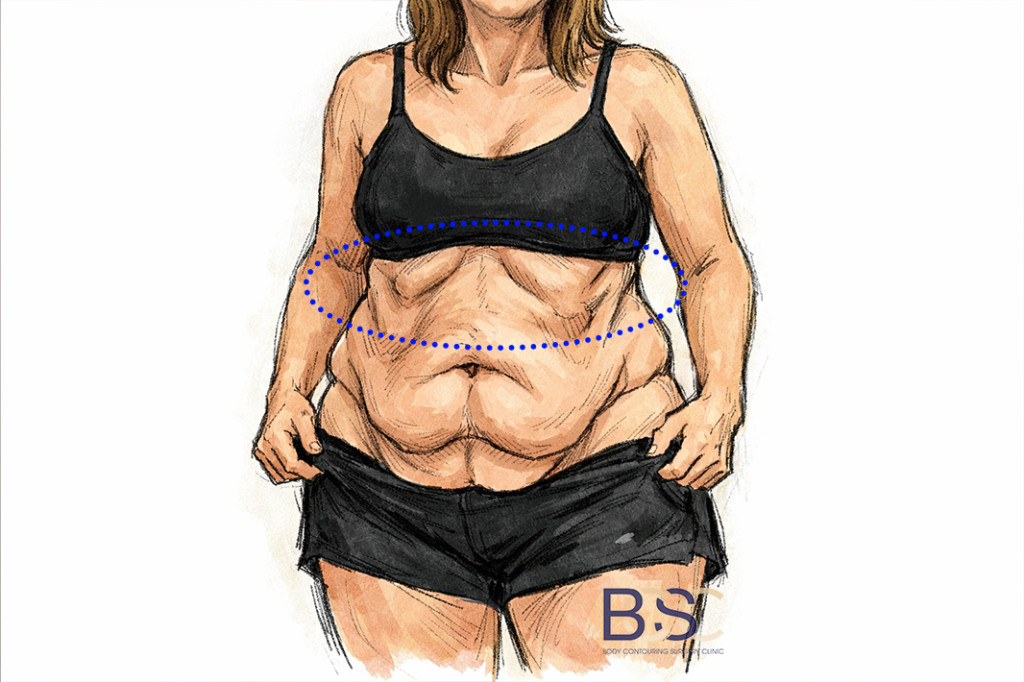
Dual Vector Abdominoplasty combines a Fleur-de-Lis abdominoplasty with an upper abdominal lipectomy in a single operation. This allows skin excision along two distinct vectors:
- A lower and central vector through the Fleur-de-Lis component
- An upper vector through the upper abdominal lipectomy
The resulting incision pattern resembles a sideways “H”, consisting of a lower abdominal horizontal incision, a vertical midline incision, and an upper abdominal horizontal incision. This configuration allows targeted removal of excess skin that may not be adequately treated with traditional techniques alone.
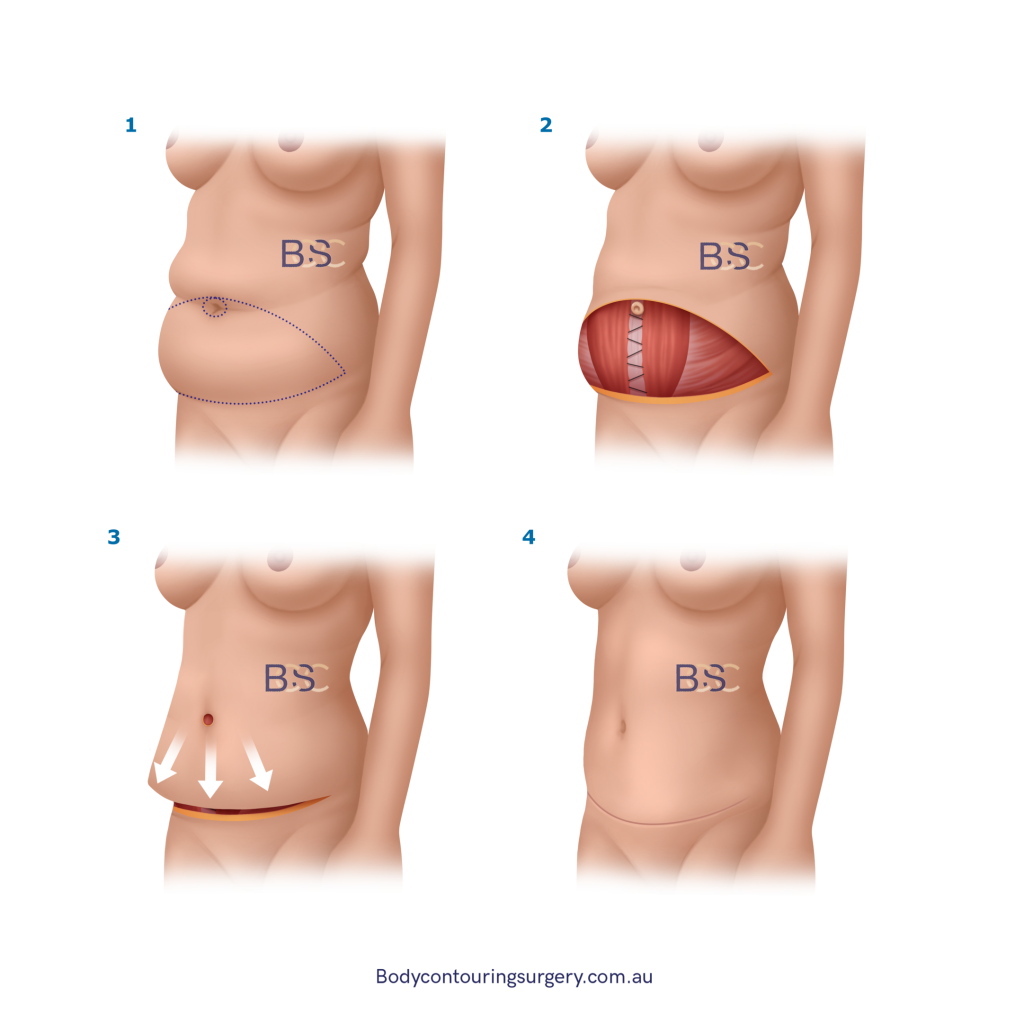
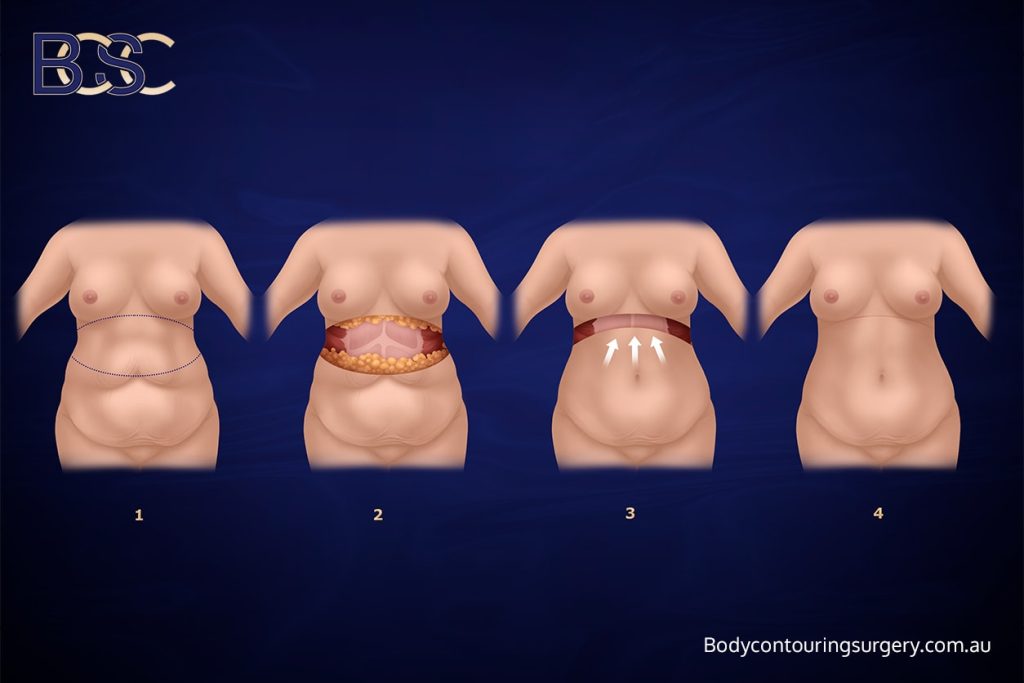
Abdominal Muscle Considerations
During abdominoplasty surgery, the abdominal muscles are assessed. If muscle separation (diastasis recti) is present, repair may be performed. Not all patients require muscle repair; this determination is made on an individual basis.
Belly Button Management
The belly button is usually preserved during abdominoplasty procedures. Its position may change as excess skin is removed and abdominal contours are adjusted. Care is taken to maintain appropriate placement relative to surrounding anatomy; however, outcomes vary among individuals.